
Every mother’s dream is to have healthy children. When she has an unwell baby, the dream turns into a lifelong nightmare.
I, Dr. Sahar Hassanein, went through this bitter experience 30 years ago, when we had a premature baby girl. She spent a week in the neonatal intensive care unit. She was different, in the first months of her life she had little sleep, and little breastfeeding. Her right hand was always closed, and she used it very little. The pediatrician didn’t realize that there was a problem. She gained motor skills later than her peers and she preferred using her left hand to reach for objects as early as 4 months of age. At the age of 9 months she was diagnosed with hemiplegic cerebral palsy (also known as congenital hemiplegia; or, weakness on one side from birth) due to presumed perinatal stroke.
Every part of the mother’s dream is affected, as hemiplegia affects every aspect of a child’s life. Her childhood, social life, and ability to play with her siblings were interrupted regularly. She had physical therapy sessions, schooling, pressure from her teachers, and bullying from her classmates. The whole family was overwhelmed with physical and mental burdens, impacting their life.
Perinatal stroke can result from damage to the brain from many causes. Perinatal strokes can occur during pregnancy, birth, or the first 28 days of life. Childhood stroke occurs after the first 28 days of life until 18 years of age. Pediatric stroke is often missed in the acute stage (when it first occurs), especially in newborns. We should suspect stroke in infants with complicated births, especially when movement between sides of the body is not the same (e.g., seizure or weakness). A brain scan should be performed as soon as possible if acute stroke is suspected. Sometimes, treatments can help the stroke, but only if performed as early as possible. We diagnose presumed perinatal stroke months or even years after an acute stroke is missed. Usually, it is diagnosed in infants with hand preference before one year of age. The brain scan will sometimes reveal a prior injury (stroke).
Parents and pediatricians should be aware that early hand preference before the age of 1 year is abnormal. Not meeting normal motor development may mean there is a problem in the baby’s nervous system. If the baby is weak on one side (arm and leg), the baby should start physical therapy to improve function. It is important to create an inclusive and supportive environment in the family and at school. Acceptance is an important part of this environment. This is a basic right for the post-stroke child and their family’s human right. Educating the child to perform their daily life activities helps the child to be independent. Creating a gym area at home for all family members is a good idea to promote exercise long-term. Playing, dancing (e.g., Zumba), drawing, painting, and sharing physical activities will improve the whole family’s mental health.
I, Shelley Dean, am a pediatric occupational therapist who specializes in the treatment and rehabilitation of children with perinatal and pediatric stroke. If you are reading this article, chances are you have a loved one that is a stroke survivor. You now know that stroke can happen at any age. However, what happens if you are the mother of an infant or child with a stroke? What do you do? No one’s journey is the same, but I’d like to share how we can all work together to support one another.
In the case of the stroke not being identified when it occurs, a parent may be the first to notice a delay in their infant’s feeding and motor skills. Unfortunately, it may be 3-6 months after birth when the child may not show good head control, may have low tone, and may not be able to sit up or use one of their hands. This is when we start to look for an explanation. This may begin with brain scans such as MRI and blood tests. Brain scans can show us the location of stroke and the neurologists will try to determine the type and timing of the stroke.
First, we gather the family and child’s story of their journey. We start from the present and look back to the birth history. We talk about the early days of pregnancy and childbirth. Sometimes, the parent may be able to remember an event where the child had a seizure or was very groggy. Rarely, there was a problem at birth involving apnea or anoxia (trouble with oxygen supply). Sometimes we do not know the timing or cause of the stroke. Unfortunately, perinatal and childhood strokes often have risk factors we cannot change.
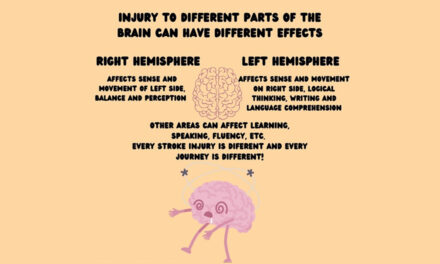
In childhood stroke, the location of the injury is valuable information. Areas of the brain control certain functions, so the type of problems a patient may have can help us know where the injury might be. The type of stroke is also very useful information for the child’s prognosis. For example, hemorrhagic strokes (too much blood causing a bleed) have different causes than ischemic strokes. Ischemic strokes are often caused by decreased blood flow in arteries. Knowing the cause of stroke (for example, heart or blood problems) may change the care plan. Depending on the cause of the initial stroke, a child may be at higher risk of a future stroke.
The role of the occupational therapist is to create a plan of care that promotes recovery. We also want to lessen the impact of the stroke on the child’s overall abilities. This may include feeding, hand use, play, posture, speech, vision, attention, and thinking. Therapies are based on the child’s age, current abilities, and cultural and familial factors. Below are examples of how we approach children with pediatric stroke.
0-11 months: We do therapy at home to address posture, play and feeding.
12 months to 24 months: We do therapy at home and in the clinic setting. We address self-care, feeding, posture, tone, play and developmental milestones. We can introduce equipment to help with adapting. We can use splinting and orthotics (braces like SupraMalleolar Orthotics [SMOs] or Ankle Foot Orthotics [AFOs]).
25 months to 48 months: We discuss peer modeling. We do therapies in a community day care setting and clinic setting. We also visit the home to talk about home exercises to continue therapy at home. We start to work on home programming of swimming and bilateral integration sequencing.
4 -12 years: We do therapy in clinic and community settings with physiatry and neurology. We work on home programming and community integration of swimming, sports, and bike riding. We continue to work on home exercises.
We hope you have benefited from hearing the stories of our journey. Every child is different, but together at IPSO, we support you on your journey.
About the Authors

Shelley Dean OTD, OTR/L
Pediatric Occupational Therapist
Email: shelley@crosswaytherapy.com

Sahar M. A. Hassanein, MD
Pediatric Neurologist & Professor of Pediatric Neurology
Faculty of Medicine, Ain Shams University, Cairo, Egypt
Dr. Sahar Hassanein is the owner and founder of “National Registry for Egyptian Pediatric Treating Neuromuscular Diseases” EGYPT PED NMD, and National Egyptian Network Pediatric Stroke and Hemiplegia Registry “NENPSHR”. Dr. Hassanein is Board Member and Secretary of African Child Neurology Society (ACNA). She currently serves on the Executive Committee of the International Pediatric Stroke Study (IPSS) and is an Educational Committee Member of the International Pediatric Stroke Organization (IPSO). She is also the Editor-in-Chief of IPSO Kid Stroke Connections. Dr. Hassanein’s research interests include neonatal and pediatric neurology, perinatal asphyxia and HIE, neural repair, neuromuscular and pediatric stroke.
Graphics: Shelley Dean, OTD, OTR/L, Sahar Hassanein, MD and Sarah Wagdy
Medical Editor: Kevin O’ Connor, MD
Community Editor: Jalaia Jackson


{kind=link}